|
|
|
|
|
|
|
Importance of Subject.—The diseases of the eye are so important, and serious injury or loss of the organs of vision is such a terrible misfortune, that they demand a careful consideration. For the better comprehension of this group it will be needful, however, to give some preliminary explanations in regard to the eye, and also the ear and nose, with their appendages.
Wonders of the Eye.—The eye is probably the most wonderfully ingenious and complex organ of the human body, and being proportionately delicate, requires to be guarded with the greatest care. Few catastrophes are more grievous than that of total blindness, and most people would rather lose all the other senses than be deprived of sight.
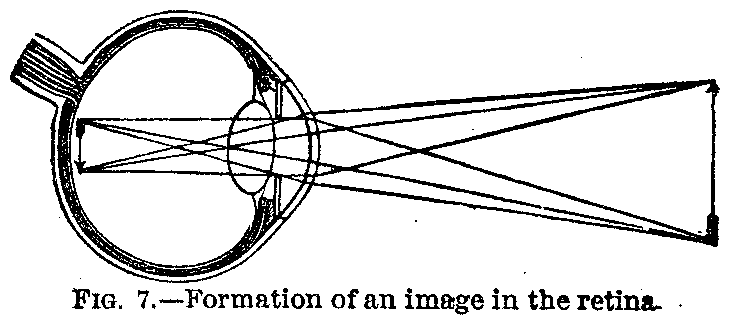
Structure of the Eye.—The intricate structure of the eye may perhaps be best comprehended if we remember that its general plan is that of a photographer's camera, the convex glass in the front of which corresponds with the crystalline lens of the eye, a picture of external objects being formed upon the artist's ground-glass plate in the one case, and upon the retina at the back part of the eyeball in the other.
The Retina.—Now, the retina is simply the expanded optic nerve, which has the peculiar power of perceiving lights or colors, and the chief difference between the eye and the camera is, that in the former temporary impressions only are perceived by the brain, through the optic nerve and retina, and in the latter instrument these temporary impressions are intended to be rendered permanent on the sensitive plate or paper, as a photographic picture.
The Eye Socket.—The eye is carefully protected from accidental injury by being embedded in a deep cavity or socket in the solid bones of the face and head, which guard it jealously from attack on either side and at the back. This socket is much larger than the eye itself, and the bony cavity is filled up behind and at the sides of the eyeball with an admirable cushion and packing of soft fat.
|
|
|
|
|
|
|
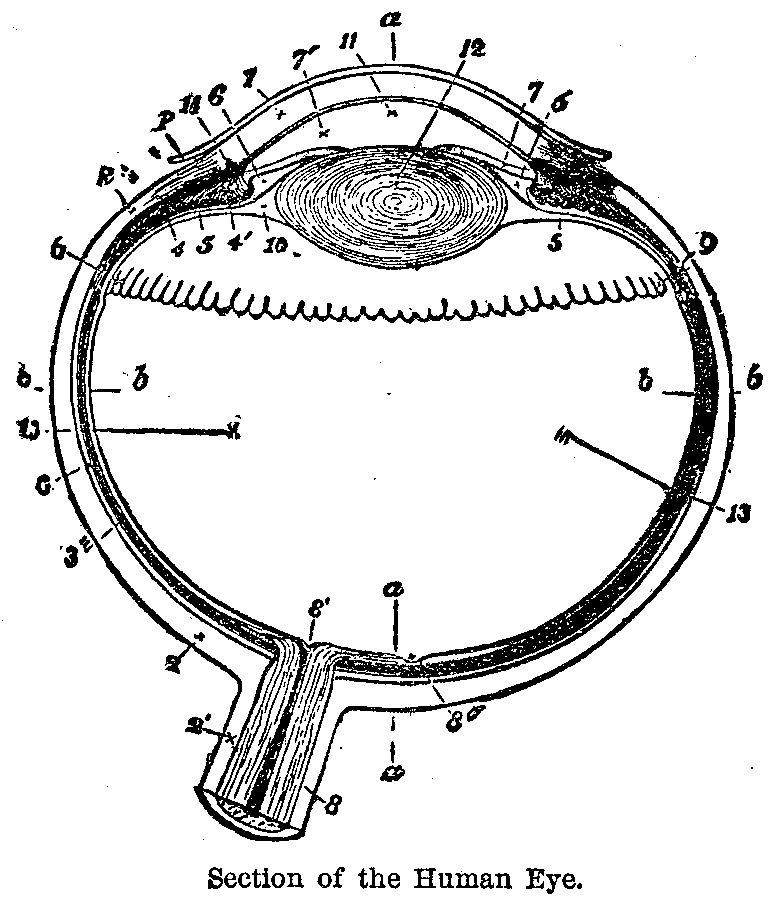
The Cornea.—The eye itself, as can be readily seen in that of a pig or sheep from a butcher's shop, is a white ball almost exactly round, except where the clear circle projects a little in front. This clear part, called the cornea (1), is as transparent as glass, and is set in the space made for it in the white part of the eyeball, very much as a watch crystal is set in its frame. The white portion of the ball, called the sclerotic coat (2), is a tough membrane, very strong and dense, which gives shape to the organ of vision, and protects the extremely delicate structures within. The cornea and sclerotic coat each average about one-twentieth of an inch in thickness.
The Iris.—Inside of the cornea is a circular curtain, with a round hole in the middle, called the iris (7), so named because it varies so much in color, being frequently blue in blonde individuals, and brown or black in brunettes.
The Pupil.—The round hole in the centre of the iris is called the pupil, and is the black spot seen on looking into a person's eye. This spot varies in size according to the amount of light, being larger in the shade and smaller in bright sunshine. In human beings it always remains round, unless the iris is diseased, but in the cat, for example, it changes its shape, becoming a narrow slit in a strong light.
Use of the Iris.—This closing up of that curious curtain, the iris, is a beautiful provision for shutting off an excessive amount of light, which would otherwise pass through the pupil in too great quantity, and irritate the sensitive parts of the organ of vision within.
The Sclerotic Coat.—The sclerotic coat is lined on its inside with a thin layer of black membrane, called the choroid coat (8), which seems to have almost exactly the same object as the black lining of the photographer's camera, namely to absorb any extra rays of light, and so prevent the picture from being indistinct.
|
|
|
|
|
|
|
Structure of Retina.—Inside of the choroid coat, and immediately in contact with it, lies the retina, a third hollow ball, made up of an expansion of the optic nerve, which enters the eye at the back (8), through openings in the sclerotic and choroid coats. The retina is made up of several layers, the outermost of which is formed by the terminations of the nerve-fibres in what are called the rods and cones of vision. These rods and cones are so wonderfully sensitive that through them we can perceive the differences of color and outline in the images of objects formed within the eye. They therefore correspond to the sensitive plate in the camera of a photographer.
Other Portions of the Eye.—The remaining portions of the eye are chiefly useful in forming this image of which we take cognizance, and act upon the light exactly as the lenses of an opera-glass or of a camera do, except that they are provided with a more convenient way of changing the focus as may be required. The first of these which the light reaches, after it penetrates the cornea, is the crystalline lens (12).
Crystalline lens.—This lens can be readily seen by squeezing it out of the eye of a pig or sheep after death, is very much like a large dewdrop or rounded diamond, in size, shape and general appearance, and is solid enough to bear gentle handling. It has the form of a small, thick magnifying glass or lens, and if held over the letters of a printed book, is at once seen to have the same power of making objects seen through it look larger.
Position of Crystalline Lens.—The crystalline lens is placed in the eyeball a little behind the iris, and is large enough to extend out beyond the edge of the pupil, unless that opening in the curtain is wider than usual. If it were not so perfectly transparent we could see the crystalline lens every time we looked a person straight in the eyes, as is shown in cases of cataract, a disease where the lens becomes first milky and then opaque, so that its position can easily be recognized, and the edge of the iris seen to move over it, as the pupil expands and contracts under the influence of varying degrees of light.
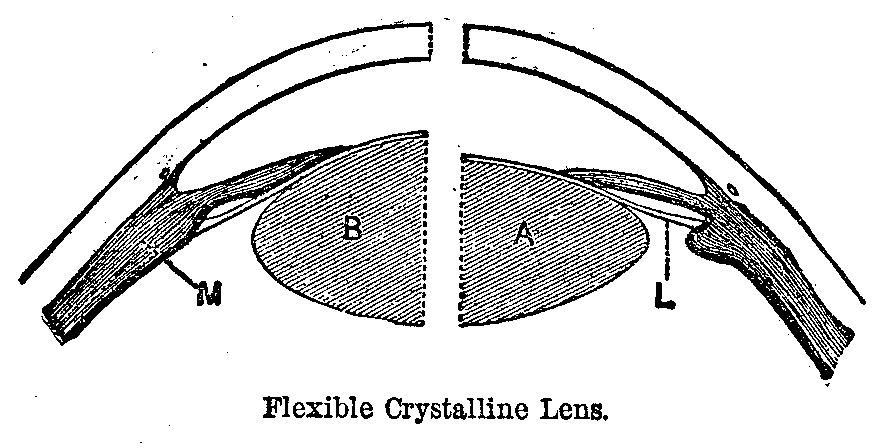
Arrangement of Focus.—Every one who has looked much through a telescope, or opera-glass, knows that a different arrangement of focus is needed to show a near and distant object clearly, and that this altered focus is obtained by adjusting the relative position of the component lenses. In the living eye, nature contrives to obtain this necessary effect of two or more lenses with a single one, by making that one (the crystalline) soft enough to change its shape a little, as shown in the diagram, and then providing a muscle called the ciliary muscle (M), through the action of which the lens may become more convex, that is rounded (as at B), and so enable us to see near objects more distinctly. It is the mechanical effort required to keep this little muscle constantly on the stretch that causes the eyes to feel so tired after long application over reading small print or doing fine work of any kind. Hence, avoidance of too prolonged a strain of this nature is an important part of the hygienic care of the sight, on account of such a tendency as exists to exhaust the power of this muscle.
|
|
|
|
|
|
|
The Aqueous Humor.—The space between the crystalline lens and the cornea is filled by the aqueous humor (11), a watery fluid bathing the front and back of the iris, which, floating thus in a clear, transparent fluid, has an opportunity to move with entire freedom, and so most perfectly perform its duty as a curtain to shut off any excess of light whenever there is danger of a superabundance injuring the sensitive retina within. The aqueous humor, being shut in by the convex cornea, must, of course, take the shape of that clear membrane, and, forming with it a convex lens, still further aids the crystalline body in bringing the rays of light to a focus upon the retina, and so forming a sharp image upon that sensitive membrane.
Action of Aqueous Humor.—The action of the aqueous humor in this instance is precisely similar to that of water poured into a glass globe standing in the sunshine. Whilst the globe is empty, it has but little effect in concentrating the sun's rays into a focus, but when filled with water, its power as a lens is considerable, and it may even operate so energetically as a burning-glass as to set fire to inflammable substances placed at a proper distance. Want of suitable curvature, and also in many cases the fact of its being curved unequally in different directions, by making the lens or magnifying glass too strong or too weak, has much to do with causing imperfect sight.
Vitreous Humor.—The chief bulk of the eye is made up of the vitreous humor, which receives its name from its vitreous or glassy appearance. This fluid is contained in the cavity of the retina, and has running through it numerous, fine, interlacing fibres, as transparent as itself, which probably help to prevent the delicate retina from being injured by its shaking about during violent movements of the head and body.
|
|
|
|
|
|
|
Duty of Vitreous Humor.—The vitreous humor has little or no share in aiding to form the image upon the retina, but does perform an important duty in keeping the globe distended, so that in a sound eye the retina is held at the exact distance, where it can receive images of objects cast upon it in their sharpest and best defined condition.
How to Understand the Eye.—An excellent way to understand fully how the eye acts as an optical instrument, is to actually make a camera of the eye of an ox or other large animal, by cutting away the sclerotic coat at the back part, and then shading this in a small box for instance, so that the images formed by cornea and crystalline lens can be seen inverted upon the translucent retina at the hinder portion of the eye.
Eye Diseases.—The diseases of the eye, according to the nomenclature here followed, are seventy-five in number, so that it is impossible properly to describe the treatment of any but the more important. Among the first of these are to be ranked the diseases of the conjunctiva.
Character.—This is an inflammation of the delicate membrane over the front of the eye, covering the whole of the cornea, and the part of the sclerotic coat or white of the eye, which is naturally visible.
Symptoms.—The usual symptoms of inflammation can nowhere be observed more distinctly than in the eye; the four great characters of this morbid process, as described by Celsus, about the beginning of the first century, being very apparent. Here, as elsewhere, redness, heat, pain and swelling are the indications of inflammation, just as they were in the days of the old Roman physician, more than eighteen hundred years ago. The redness of the eye in this affection varies with the, intensity assumed, but in severe cases it may completely obscure the white of the eye, so that the whole surface, except the cornea, appears quite red. The pain and burning heat of the eye are sometimes almost unendurable.
The Swelling.—The swelling of the conjunctiva is often so considerable as to rise up all round the edge of the cornea, and this projection of the inflamed membrane may be so great as to prevent the eyelids from being closed. Intolerance of light and profuse flow of tears, the latter resulting from irritation sympathetically extended to the lachrymal gland, which supplies those persuasive drops of salt-water, are common symptoms in some forms.
|
|
|
|
|
|
|
Catarrhal Conjunctivitis.—Catarrhal conjunctivitis or catarrhal ophthalmia, as it is also named, is the form of this affection usually produced by cold. Redness and pain, as if a particle of dust had got into the eye, with a free discharge of water, are the first symptoms. Intolerance of light is not very great, unless the cornea becomes involved. Vision may be slightly obscured, but is seldom seriously affected.
Treatment 1.—The treatment consists of active purgation with calomel (one-tenth to one-fifth of a grain every hour until one to two grains are taken), followed by epsom or rochelle salts. Soothing lotions to the eye, as for example, that of sassafras pith with a very little extract of belladonna to begin with, and, after a day or two, applications of weak solutions of lunar caustic (silver nitrate) should be used.
Rx.---Silver nitrate ............................... 15 grains
Distilled water ............................. 1 ounce
Mix. Directions:---Apply to the inner eyelids with a
little cotton wrapped on a toothpick or a match-stick.
The application should be made once a day for several days, and although the caustic solution smarts severely at first, it leaves, after fifteen or twenty minutes, an astonishing feeling of relief to the affected organ, and in favorable cases rapidly reduces the inflammatory action.
2. To prevent the eyelids from adhering during sleep, and so aggravating the trouble when pulled apart in the morning, an ointment should be used, preferably that recommended by Professor Pegensticker, which is a favorite of most physicians. The formula is:
Rx.---Yellow oxide of mercury..................... 1 grain
Vaseline or cosmoline........................ 1 ounce
Mix thoroughly, and apply lightly to inner eyelids night
and morning.
3. In many cases "ordinary salt and water or a 2 per cent. solution of boric acid will suffice to effect a cure. Simple conjunctivitis of a chronic nature is often associated with catarrh of the nasal mucous membrane, and may be cured by correcting the catarrh of the membrane." (Professor Weeks.)
Pustular Ophthalmia.—This, called also phlyctaenular conjunctivitis and strumous ophthalmia, is the form in which the scrofulous predisposition to disease is very apt to manifest itself in young children. It is almost always accompanied with an eczema of the head or face.
|
|
|
|
|
|
|
Treatment.—In this affection general treatment for the constitutional disease is the most important. The patient should be placed in the best hygienic surroundings. The eyes should be kept clean with an antiseptic solution, as a 2 per cent. boric acid wash, and the yellow oxide of mercury ointment, mentioned above, rubbed into the eye once or twice daily.
Purulent Ophthalmia.—This is a more violent and contagious form of conjunctivitis, in which the sight is sometimes seriously endangered. The discharge of thick yellow pus or matter is abundant, and the inflammation sometimes progresses with great rapidity.
Treatment.—Active purgation, leeching followed by blisters behind the ears, and application of the stronger solutions of nitrate of silver, are often necessary to preserve the sight. In the contagious variety great care must be taken to avoid conveying the disease from the sick to the well by the use of soiled towels, handkerchiefs, and so forth.
Spread of the Infection.—In bad cases it is probable that the infection may occur by being wafted along in the atmosphere through a large room, or even through a whole house, as is seen sometimes in boarding schools and children's infirmaries.
Purulent Ophthalmia of Infants (ophthalmia neonatorum).—This is another contagious form of the disease, affecting new-born children and, if not properly attended to, destroying their sight. It is the result of an infection with the gonococcus which Niesser discovered in 1879 to be the cause of gonorrhea. The inflammation develops in less than three days after birth.
Symptoms.—First there is redness and irritability of the conjunctiva.
2. In about twenty-four hours an excessive secretion of tears and a whitish discharge appears.
3. This is followed later by a swelling of the lids and of the conjunctiva and a change in the character of the discharge from a whitish to a yellow, purulent type.
4. The child suffers very little at first, but later, when the discharge becomes more plentiful and thinner, the patient loses his appetite, is restless and suffers a great deal of pain.
Treatment.—The treatment is divided into two classes. 1. Prophylactic or preventive; and, 2. Curative.
1. That prophylaxis is possible was demonstrated by Crede, a noted obstetrician of Bonn, who reduced the percentage of these cases in the wards of his hospital from 13 per cent. to less than 2 per cent.
Application of the Treatment.—This he accomplished by dropping one or two drops of a 2 per cent. solution of nitrate of silver in the eyes of new-born infants. This procedure is commanded by law in some communities. American authorities only recommend it where the birth canal is presumed or known to be affected.
|
|
|
|
|
|
|
Analysis of Prophylactic Treatment.—The Cyclopedia of Medicine and Surgery (Gould and Pyle) says: The prophylactic treatment consists:
1. In removing the disease from the mother before labor if possible.
2. Thorough disinfection of the vagina before labor with solution of creolin, carbolic acid, boric acid, salicylic acid, mercuric chloride or other antiseptic.
3. Thorough disinfection of the child's eyes as soon as born.
These precautions should be carried out in all suspicious cases.
2. Curative Treatment.—After the disease has made its appearance, the most strenuous efforts and the most unceasing vigilance and care are demanded to prevent a partial or total loss of sight. Many of the blind we see about us, for whom we feel so much sympathy, can blame their unfortunate condition upon the lack of treatment in the first few days of their lives.
If possible a physician should be summoned at once and his orders followed implicitly, and it may be necessary for him to see the child several times a day to make the necessary applications.
Rules for Treatment.—If a physician can not be had, thorough attention to the following rules will probably result in a cure:
1. Cold applications which tend to lessen the amount of local inflammation.
2. Frequent and thorough flushings of the eyes with mild antiseptics, as boric acid in distilled water.
3. The application of lunar caustic (silver nitrate) ten grains in the fluid ounce of distilled water, two or three times a day.
4. If any ulcers appear on the cornea, weak yellow oxide of mercury ointment should be rubbed, thoroughly but gently, into the lids twice a day.
5. Nourishment, cleanliness and warmth must be maintained.
Diphtheritic Conjunctivitis.—This is a condition of the eye caused by an infection with diphtheria. Fortunately it is extremely rare in America.
Symptoms.—Pain is present, the lids are swollen and hard. The discharge is scanty and may be watery or a thin pus. The constitutional symptoms of diphtheria may be present.
Treatment.—Instillations of very weak solutions of atrophine will relieve the pain. Antitoxin should be administered very early. Otherwise the treatment is the same as in purulent conjunctivitis.
|
|
|
|
|
|
|
Trachoma.—Granular conjunctivitis or granular lids, is also a contagious disease of the eyes.
Symptoms.—The inner sides of the lids become rough, inflamed, and covered with little projections which irritate the cornea at every movement of the ball or lids. It seriously affects vision, and is often very obstinate, but can frequently be vastly benefited.
Treatment.—1. Perseverance in constitutional treatment.
2. Local applications of nitrate of silver solution, or sulphate of copper to the granulations.
3. Unless improvement follows soon, local treatment should be discontinued and a specialist consulted. There is rarely complete recovery.
Causes.—Keratitis or inflammation of the cornea may occur from a punctured wound of the eye, or it may be the result of the scrofulous diathesis, or even more commonly of inherited syphilis. It occasionally results in ulceration of the cornea, which sometimes perforates this structure and, allowing the humors of the eye to run out, irrevocably destroys the sight.
Treatment.—Local treatment of the accompanying conjunctivitis and the use of atropia to keep the pupil dilated, so that it, the iris, may not become involved in the inflammation, are important, but the chief reliance must be placed upon constitutional remedies for those general diseases, of which this affection of the eye is little more than a symptom. The white spot or scar left by an ulcer of the cornea is generally permanent, and not only disfigures the organ of vision, but more or less completely obscures the sight for life.
Preventive Treatment.—Since a scar of this kind is so injurious and when once fully formed can scarcely ever be removed, the ounce of prevention is of tenfold importance, and every care should be taken, by securing the most skillful treatment for ophthalmia as promptly as possible, to reduce to its smallest dimensions the danger of such a catastrophe to sight.
Symptoms.—Inflammation of the sclerotic coat, or sclerotitis, is generally characterized by the intense, deep-seated pain it causes, and by the pink hue of the white of the eye produced. The chief varieties are the rheumatic and the syphilitic.
(Continued on page pg0390)
|
|
|
|
|
|
|
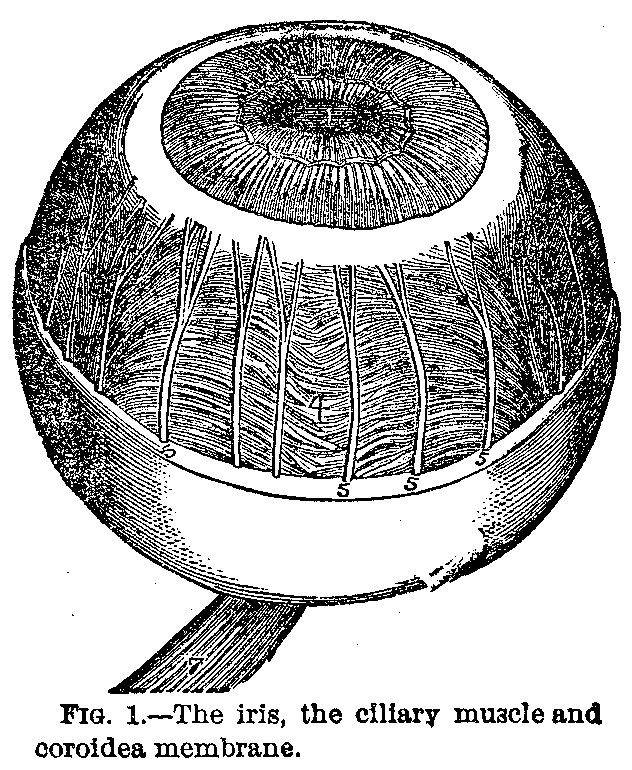
FIGURE NO. 1.---Iris, ciliary muscle and. coroidea membrane.
1. The pupil.
2. Ciliary muscle.
4. Arteries of the coroidea membrane.
5,5,5,5. Sclerotic tunic, cut circularly and removed.
7. The optic nerve.
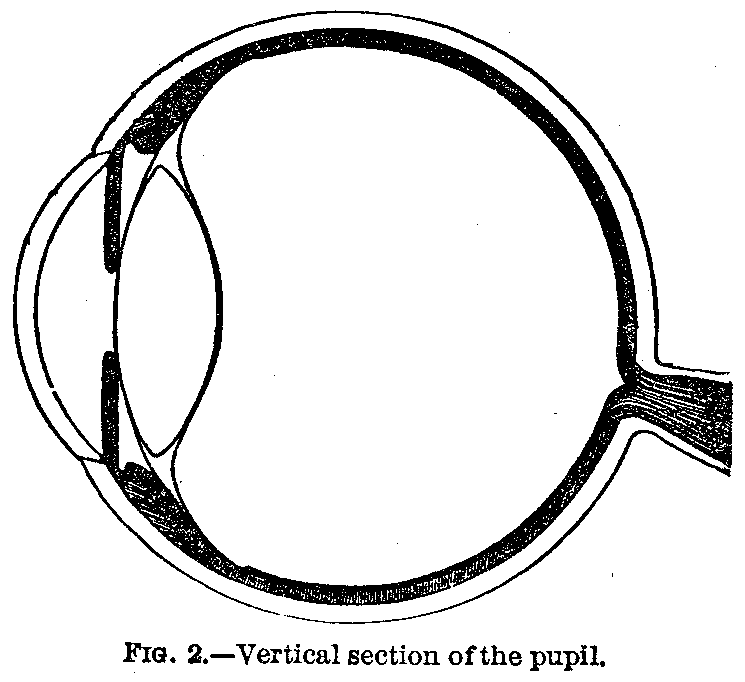
FIGURE NO. 2.---Vertical section of the pupil.
FIGURE No. 3.---Artificial eye.
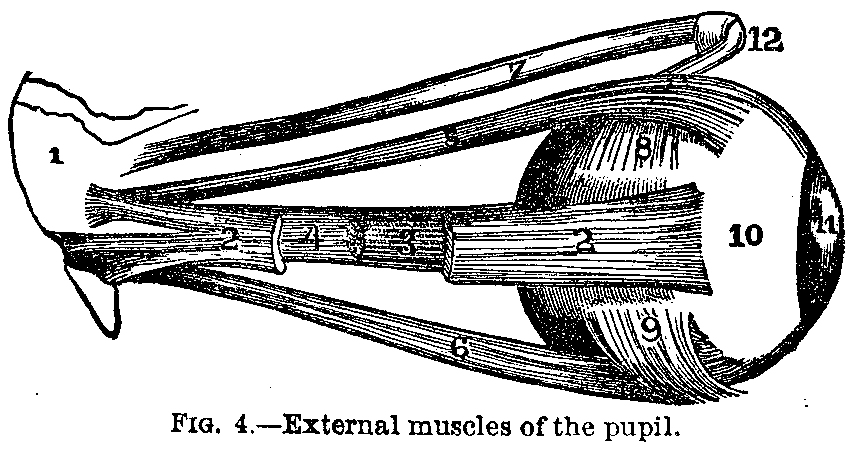
FIGURE NO. 4.---External muscles of pupil.
1. Part of the sphenoidal bone to which some muscles are attached.
2, 2. External straight muscle.
3. Optic nerve.
4. Internal straight muscle.
5. Upper straight muscle.
6. Lower straight muscle.
7. Upper oblique muscle.
8. Insertion of the upper oblique muscle of the pupil.
9. Lower oblique muscle.
10. Sclerotic tunic.
11. Cornea.
12. Cartilaginous pulley of the upper oblique muscle.
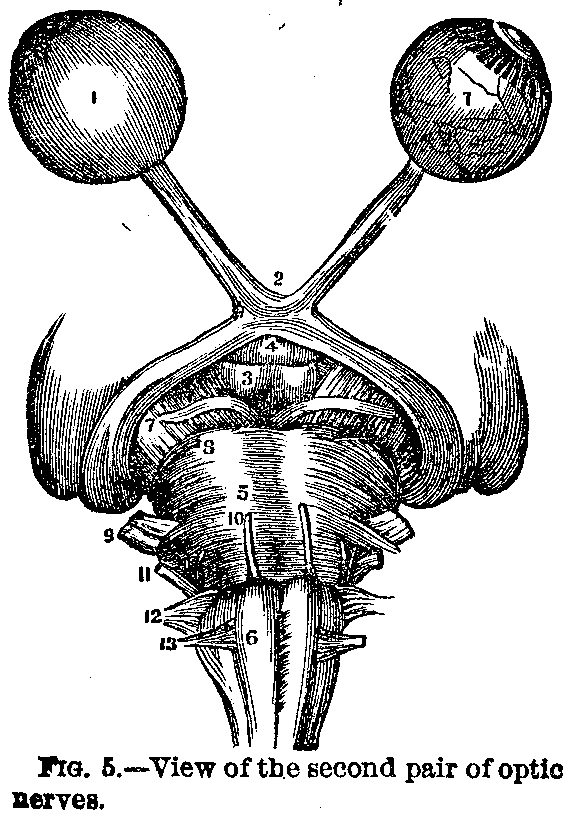
FIGURE NO. 5.---View of the second pair of optic nerves.
1,1. Globe of the eye. The left, perfect. The right one has the
sclerotic and coroidea tunics removed, showing the retina.
2. Quiasm of the optic nerve.
3. The whitish bodies.
4. The infundible.
5. Varolius bridge.
6. The medulla oblongata.
7. Third pair: motor nerves of the eye.
8. Fourth pair: pathetic.
9. Fifth pair: trigeminous.
10. Sixth pair: external motors.
11. Seventh pair: auditive and facial nerves.
12. Eighth pair: neumogastric, accessory, spinal and
glossopharyngeal.
13. Ninth pair: hypoglossus.
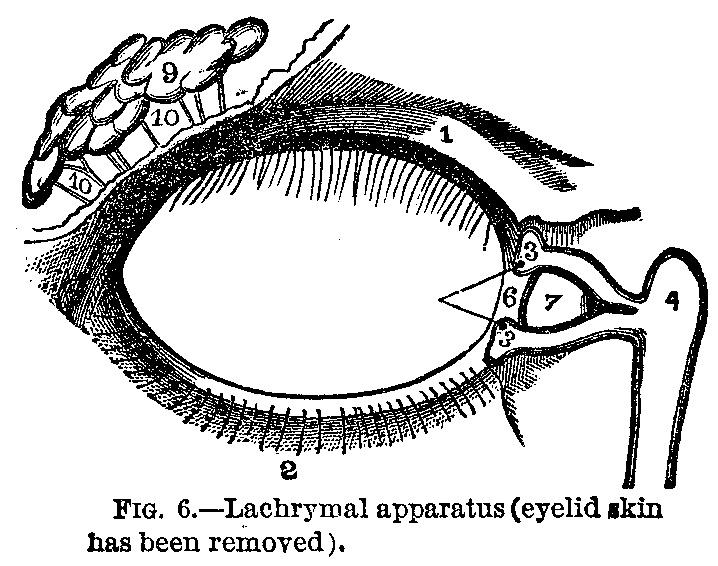
FIGURE NO. 6.---Lachrymal apparatus (the skin of the eyelid has been
removed).
1. Cartilage of the eyelid.
2. Inserion of the eyelashes.
3, 3. Lachrymal ends or openings of lachrymal canals in the eye-lids.
4. Conduit to the nose.
6. Cul-de-sac at the orbital extremity of the canal.
7. Lower corner of the eye.
9. Lachrymal gland.
10,10. Canals carrying tears to the eye.
FIGURE NO. 7.---Formation of an image on the retina.
|
|
|
|
|
|
|
For an explanation of the illustrations see text on opposite page.
|
|
|
|
|
|
|
Treatment.—The treatment is to be more especially directed towards counteracting by general remedies the poisons of these two virulent constitutional affections.
Character.—This is an inflammation of the iris, which may be simple or gouty, syphilitic or scrofulous.
Symptoms.—Its symptoms are intense pain in most cases, although in others little uneasiness is felt; change in color of the iris, contraction of the pupil, and impairment of vision. Inflammation of the iris has always possessed a great interest for physicians, because it is the only cavity lined by a serous membrane into which we have the privilege of looking and seeing what is going on when the membrane which forms its boundary is inflamed. Hence, the observation of a case of iritis is not only the most interesting, but also the most instructive, lesson in the sciences of pathology and therapeutics which nature ever vouchsafes to us, as we carefully watch the progress of the disease and the effects of medical treatment from day to day.
Treatment.—Since one of the greatest dangers of iritis is that the pupil will be drawn together by the whitish lymph infused in the inflammatory process, and, by being thus closed, shut off the sight, it is very important to keep this opening of the pupil as large as possible by the use of belladonna, or its active principle, atropia, throughout an attack of iritis. Besides this, general bleeding, or free leeching behind the ears, or on the nape of the neck, followed by repeated blistering, should be employed, and active purgatives with mercury to slight salivation contribute toward the cure. Opium by hypodermic injection to relieve the intense pain, and cool anodyne applications to the affected organ, are valuable palliatives.
Character.—This is an inflammation of the retina and seldom occurs alone. It may be due to Bright's disease, may result from a specific taint, or may be of the hemorrhagic variety. This last named condition is nearly always in the aged and is an occasional accident happening in cases where the kidneys are hard and shrunken.
Treatment.—The treatment is of course directed to the disease which causes this inflammation.
|
|
|
|
|
|
|
Causes.—This is also usually in conjunction with systemic diseases, as tuberculosis, syphilis, rheumatism and gout. The suppurative variety may be due to a blow or may be carried from some distant suppurative process.
Treatment.—The treatment is directed to the cause and is mostly general.
Character.—This is a disease of the retina dependent upon various changes of the retinal surface and ending in an inability of the nervous expansion to receive and transmit visual impressions from the outside world to the brain.
Causes—1. It may be produced by exposure of the eye for a longer or shorter period to a white, dazzling object like snow, and snow-blindness is the most familiar example of this affection.
2. It also occurs occasionally from accidents, such as lightning-stroke and blows on the head.
3. It may be due to degenerative changes in the retina following exhausting illness, or connected with sympathetic irritation.
4. Excessive use of tobacco sometimes produces it.
Treatment.—Where the cause of amaurosis can be discovered and removed, some hope of cure may be indulged, but ordinarily the melancholy fate of becoming permanently blind—as the poet Milton was rendered by this malady—awaits the patient. Of course, the earlier treatment is undertaken the better is the chance of arresting the malady before utter destruction of the sight is accomplished.
Character.—This is an inappropriate but long-established term indicating an opacity of the crystalline lens of the eye. In cataract, the lens becomes white and opaque, first at some point on its surface, or in the capsular membrane which envelops the albumenoid substance of which the lens is composed. The opacity extends, until at length the whole of the lens may be involved, and blindness rendered complete.
Development of Cataract.—The development of cataract is usually slow in its progress, except in the case of diabetic cataract, or cataract from a punctured wound, which may form in a few days. The process of becoming totally opaque is called by surgeons the ripening of the cataract, and it is customary to wait for the cataractous change or ripening to be complete before any operation is attempted for its cure.
|
|
|
|
|
|
|
Causes.—Most frequently there is some change in the vascular system supplying the lens, and to this lack of nutrition is due. Senility, diabetes mellitus, convulsions, injury, exposure and privation are the causes.
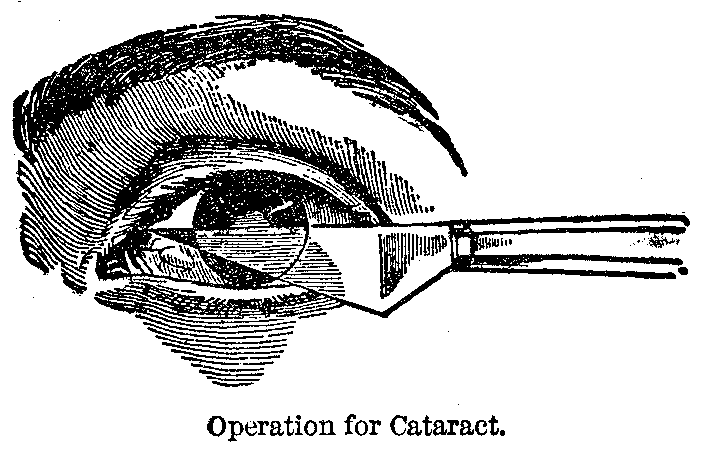
Treatment.—No medical treatment, as yet discovered, is of any avail in the treatment of cataract, but the disease may be entirely remedied by the operation of extraction, which is illustrated in the accompanying figure. As there shown, a peculiar, wedge-shaped knife, called a cataract-knife, is used to cut an opening in the edge of the cornea, through which the opaque lens is carefully drawn out, and then the eye closed up and permitted to heal.
Restoration of Vision.—When successful, as this operation proves in the hands of skillful oculists nearly nine times out of ten, useful vision is restored, and by the aid of very thick spectacles, to substitute the lost crystalline lens, the patient is often enabled to read, write or sew, as well as before being attacked with this disease. This operation of extracting the cataract is generally the most successful with the common form, which occurs in old people, where the crystalline lens is not only opaque, but hardened into a sort of horny substance.
Treatment of Other Forms.—In some of the other varieties of cataract, such as that produced by wounds or other injuries, especially in young people, the treatment by breaking up the lens with a very delicate knife, about the size of a large needle, is resorted to with success. The old-fashioned operation for cataract by couching, or reclination of the opaque crystalline lens, is now generally abandoned, as being much less satisfactory in every way than the process of extraction.
Cataract Often Hereditary.—The tendency to the formation of cataract is often hereditary, but something can be done by hygienic care of the eyes to avert, or at least to postpone, its active development. Since it has been found that operatives who use their eyes opposite to a very strong light—such as glass-blowers —are particularly liable to cataract, it is advisable to avoid such exposure as much as possible.
Effect of Electric lights.—Very probably electric lights may tend to promote the formation of cataract, unless guarded with special care. It is a curious fact, however, and one which at once disproves the fanciful theory that cataract is a disease of over-civilization and excessive study, that cataracts are frequently met with in animals, especially the horse, where the disease may often be seen in great perfection.
|
|
|
|
|
|
|
Symptoms.—This is a disease in which the most prominent symptom is an increase in the tension of the eyeball. By primary glaucoma we mean an increase in tension originating in the eye itself independent of any outside influence. Secondary glaucoma is the same condition due to an injury, some previous inflammatory process, or resulting from valvular heart disease, and so forth.
If the glaucoma is simple in character, the first symptom is partial loss of vision. In cases of inflammatory character pain may be the first feature to attract attention and may be much more severe at times.
Predisposing factors are heredity, excesses of various kinds, gouty or rheumatic tendencies.
Treatment.—Medical treatment is of value in some primary cases. Warm applications may ease the pain, or instillation of one-quarter to one per cent. solution of eserine. Operative measures of various kinds may be necessary from iridectomy to complete removal of the globe.
Weak or enfeebled sight, though a term in familiar use, is not easily defined as specially connected with any constant change in the eyeball.
Causes.—It may be due to an irritable condition of the retina, or to an impoverished state of the blood. More frequently, perhaps, it arises from a want of power to keep up the accommodation of the eye for distances, to nervous anxiety about the sight, or to the commencement of one of the serious organic diseases about the eye and its appendages.
Treatment.—Except in the latter case, much can be done by treatment, using general and local tonics, and by care of the eyes in the mode to be pointed out in the next article.
Character.—This is a very common condition of vision in which, from the greater convexity or improper position of the lenses of the eyeball, the focus of parallel rays of light does not fall upon the retina, but at some point in the vitreous humor. This error of development, as it often is, will be better comprehended, by the aid of the annexed figure, in which is shown a diagram of the eyeball and the course of the rays of light, to form a clear and distinct image of the arrow, on the retina at b, b. If, however, the eyeball is elongated, so that the retina occupies the position of the line marked 3, as is often found to be the case in near-sighted persons, it is obvious that the rays of light will have passed their true focus, and consequently when they reach the retina in this wrong position can only give a blurred and indistinct image of the object.
|
|
|
|
|
|
|
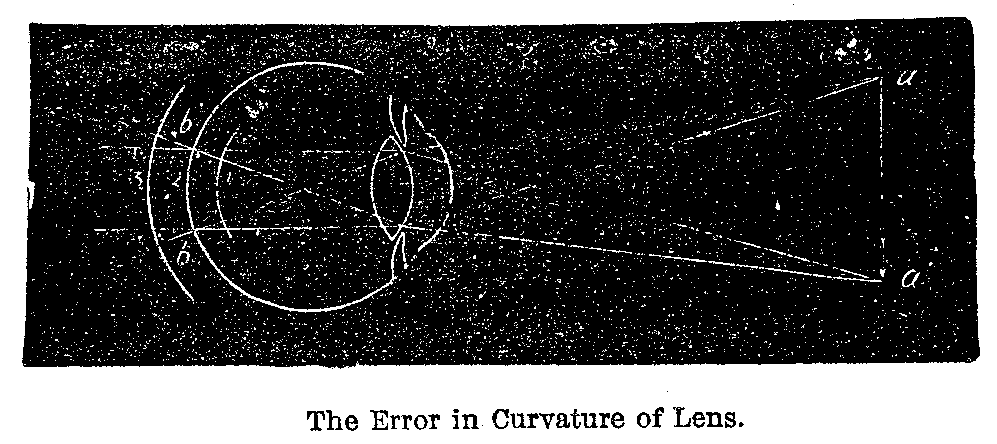
Remedy.—The remedy for myopia is the use of a concave glass, accurately adapted to the particular eye for which it is employed, and just strong enough to render the rays of light so divergent when they strike the cornea that they will be brought to an exact focus upon the misplaced retina, in its unnatural position, making in this way one error precisely counterbalance the other.
Application of the Remedy.—This remedy should by all means be applied even in early youth, in order to prevent the effort of accommodation, the straining of the eye to see as much as other children do at school and elsewhere, from not only increasing the myopia, but laying the foundation of more serious disease and ultimately, perhaps, destroying the sight.
Increase of Short-Sightedness.—The alarming increase of myopia, and especially its prevalence among young people of both sexes in city schools, must have caused many observant biologists to speculate as to the exact mechanism by which the unfavorable influences of our present civilization were at work so as to bring about this rapid deterioration of the visual organs in the last few generations of mankind.
Myopia Hereditary.—There is no doubt also that myopia is hereditary, and that according to the great law of "the extinction of the unfit," the children of myopic parents are predisposed to the development of this disease. Hence they will almost certainly suffer from it if they are exposed to conditions which would be apt to engender near-sightedness in healthy eyes, free from any taint of hereditary tendency.
|
|
|
|
|
|
|
Preventive Measures.—Among the general conclusions arrived at by scientists for aiding in this object, so important to the rising generation, the following are worthy of especial notice:
1. In the first place, study-rooms should be well-lighted during the day, and especially toward evening, because a feeble or badly-arranged light compels us to diminish the distance between the eye and the book whilst reading or writing.
2. Light should be allowed to enter from the left side. Illumination from the front is more or less dazzling, and obliges the pupils to bend forward too much, or to sit sidewise in constrained and fatiguing positions. Again, light coming from behind is entirely insufficient, because in great measure cut off by the head and upper part of the body of each scholar.
3. The windows of a school-room should be large and high, and be arranged along the left side of the apartment, so as to shed the light upon desks placed in rows, at right angles to the wall in which the windows are cut.
4. The light from above, furnished by a skylight, is not so good as that derived from lateral illumination. The light of lamps is recommended as being preferable to gas, and the gaslight shining through ground-glass globes is condemned as being particularly objectionable.
5. The inclination of the desk at which the pupil sits to read or write is a matter of no small importance. Desks which are horizontal, or only slightly inclined, favor the development of myopia, by compelling the scholar to bend the head over a good deal whilst reading or writing. Such a position brings on, as a result of mere weight of the blood, passive congestion of the head and eyes, and this in turn results in an intra-ocular tension, insensible, perhaps, when it first appears, but very marked in its effects when long and constantly continued.
Children's School Desks.—Besides, a child who acquires the habit of leaning forward in this manner is very apt to bend nearer and nearer his book, as the muscles of his back become fatigued, and thus, by straining his power of accommodation at short focus, promote the rapid development of myopia. The desks of school children should therefore be sharply inclined at an angle of 40 degrees or 45 degrees when used for reading, and their seats should not be too high, and should be furnished with comfortable backs.
6. Great care should be taken to secure school-books well printed in large, clear type; since those printed in small, indistinct letters, upon bad paper, with poor ink, as is the case with too many of the classics and the dictionaries in common use, necessitate a close approximation of the eyes to the page, and consequently exaggerated efforts at accommodation, favoring myopia. Furthermore, all punishments of school children which consist in depriving them of recreation or exercise out of doors, or in adding to their amount of study, and consequent employment of the visual apparatus, should be relinquished.
|
|
|
|
|
|
|
Faults of School Furniture.—The general principles which must be kept in view in the construction of seats and desks for school children, according to the investigations of Cohn and others, may be expressed as follows:
The faults of school furniture which give rise to injurious postures, and so conduce both to myopia and asthenopia, as well as to scoliosis or lateral curvature of the spine, are:
1. Want of, or unsuitable, backs.
2. Too great a distance between the seat and the desk.
3. Disproportion, generally too great a difference between the height of the seat and that of the desk.
4. Wrong form and slope of the desk.
Ideal School Desks.—Dr. Liebreich gives a very clear exposition of the way in which these defects cause the diseases already mentioned, and concludes with the subjoined recommendations, which he considers, however, less advantageous than what he calls the American plan of having the seat and desk made to every child's measure, or the Swiss system, where seven or more different sizes of seats and desks are manufactured to suit the different classes:
1. One and the same size and model of desk should be used for children and grown-up persons of both sexes.
2. The adaptation to the height of each child should be effected by varying the height of the seat and the footboard.
3. The edge of the table is always to be in a perpendicular line above that of the seat.
4. No seat is to be without a back, and the top of this is always to be one inch lower than the edge of the table for boys, and one inch higher than the edge of the table for girls.
5. In all classes where the boys change places the height of the seat is to be regulated in proportion to the average height of the pupils.
6. In all girls' schools, in all those boys' schools where the children do not change places, in boarding schools, and in private school-rooms, the seat of each child should be accurately regulated in proportion to its height.
|
|
|
|
|
|
|
Back Support, Etc.—The support for the back should incline only a few degrees from the perpendicular, and be so arranged as to press upon the spinal column just above the hips of the pupil. The breadth of the seat should be considerable, in order to support most of the thighs, and its height just such as to allow the feet to rest easily upon the footboard. The desk should be so arranged, by means of a hinged flap or otherwise, as to hold the book at an angle of 40 degrees or 45 degrees whilst reading, and the paper at an angle of 20 degrees whilst writing is being performed by the scholars.
Definition.—This term is applied to a defect of sight due to a difference in the curves of the cornea and crystalline lens in different directions; that is to say, the cornea, for example, may be so curved in the direction of a horizontal line through it as to have a focus of one inch, and be so much less curved on a perpendicular line that its focus in that direction is an inch and a quarter. The result of this different refraction, in different meridians of the globe of the eye, is necessarily an indistinctness of vision, because all the rays of light entering the eye from a bright point are not brought precisely to a point again upon the retina as they should be.
Treatment.—This defect, which is found to be exceedingly common, especially in myopic eyes, can be very accurately corrected by the use of properly adjusted cylindrical glasses, which are so arranged as to distort the rays of light before they enter the eye just enough in a contrary direction to cause them to be brought to an exact focus by the imperfect cornea and crystalline lens of the astigmatic eye.
Use of Spectacles.—Spectacles giving this compensation ought to be procured and faithfully worn, not only because their use will tend to preserve the eyes, which would otherwise be apt to grow strained in the effort to make up for this defect by accommodating the lens, but also on account of the headache which is often the result of such constant effort to adapt the eye to clearer vision.
Day-Blindness.—Day-blindness is a term used to describe a disease in which the person affected can only see when the light is subdued, as in the twilight.
Night-Blindness.—Night-blindness, on the contrary, indicates a condition in which there is indistinctness of vision, except in a bright light.
|
|
|
|
|
|
|
Causes.—The causes of these two conditions are not very well understood, but night-blindness is known to chiefly affect those who have used their eyes too long and too steadily in a brilliant illumination or who have been exposed to intense or sparkling light.
Treatment.—Rest is the chief means of cure, but prevention of these diseases by the proper protection of the organs of vision by colored glasses, or by the mechanical appliances mentioned when speaking of light, is infinitely preferable.
CHaracter.—The lachrymal gland, which supplies the tears, and is situated at the upper and outer angle of the eye, is subject to inflammation and the usual structural changes which result from that process. The most common disease, however, connected with the lachrymal apparatus is obstruction of the lachrymal duct or tube, which runs from the inner corners of the eyelids down into the cavity of the nose, and conveys the tears into the nasal cavity, which, under ordinary circumstances, they merely serve to keep comfortably moist.
Causes.—This obstruction may result from inflammation of the lining membrane of the duct caused, perhaps, by cold or brought about by acute or chronic inflammations of the nasal chambers. If neglected, abscess may result requiring surgical interference.
Treatment.—In its incipiency attention to the nasal passages and correction of the deformities and catarrhal condition there may suffice to effect a cure of the constriction of the duct. While acutely inflamed, anodyne lotions, as lead water and laudanum, cold or hot applications should be faithfully tried. When dilatation of the duct is demanded it should be continued until a cure is effected.
A stye is a little boil at the edge of the lid.
Causes.—When styes recur, refractive errors should be at once suspected and corrected. Ill health favors a stye as it does boils in other localities. Uncleanliness is sometimes the cause.
Symptoms.—These are so well known that it is not necessary to go into them. Suffice it to say that when a yellow spot is discernible on the stye, it is ripe and should be opened.
|
|
|
|
|
|
|
Treatment.—To hasten the pointing of a stye, apply hot compresses for fifteen minutes every two hours. Tonics are indicated in the debilitated; glasses—properly fitted—should be worn, and a boric acid eyewash used until long after the stye has disappeared.
Dangers.—This is the name for that growing in of the eyelashes, commonly known as wild hairs in the eye. Even one of these hairs, by rubbing upon the sensitive cornea whenever the patient winks, may cause much irritation and even injury to the sight.
Treatment.—Temporary relief is afforded by pulling out the offending hairs with small tweezers, but often a surgical operation is necessary to accomplish a permanent cure.
Character.—This disease is the commonest of the derangements of the eyeballs within their orbits. In it the eye is involuntarily drawn from its straight position to one or the other side, so that the natural and agreeable parallelism of its axis with that of its fellow is not maintained. When the eyes are turned in toward the nose, as is more commonly the case, the strabismus is called convergent, and when the squint is outward, it is spoken of as divergent strabismus.
Causes.—This defect is due either to shortening of one of the six little muscles by which the eyes are moved in their sockets, or to the spasmodic contraction of one of these muscles, or to paralysis of one of them and relative over-action of its natural opponent. Strabismus is in some cases an acquired affection, and may even result from the bad habit among children of imitating deformities of this kind. More frequently it appears to be the product of hereditary tendency. It may affect both eyes in the same person, and even in the same direction, and is then called double strabismus, or it may be confined to one eye, the other remaining perfectly healthy.
Treatment.—Something can be done in the treatment of this malady when it first commences in children who are not too young to wear spectacles by having these arranged with half pieces of black glass, so that the patient is compelled to look straight forward. But the simple operation of cutting through a part or the whole of the contracted muscle is in suitable cases the best remedy, and often, not always, proves perfectly successful in removing the deformity.
|
|
|
|
|
|
|
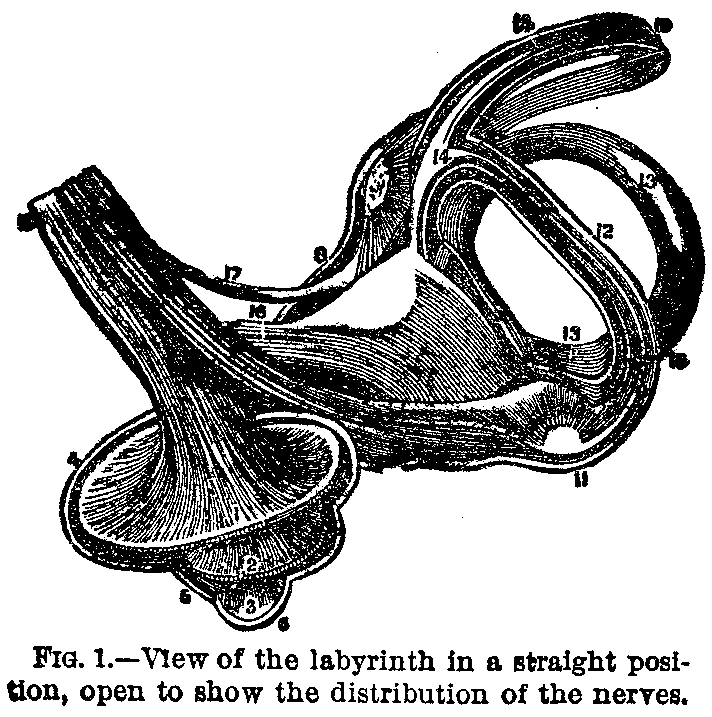
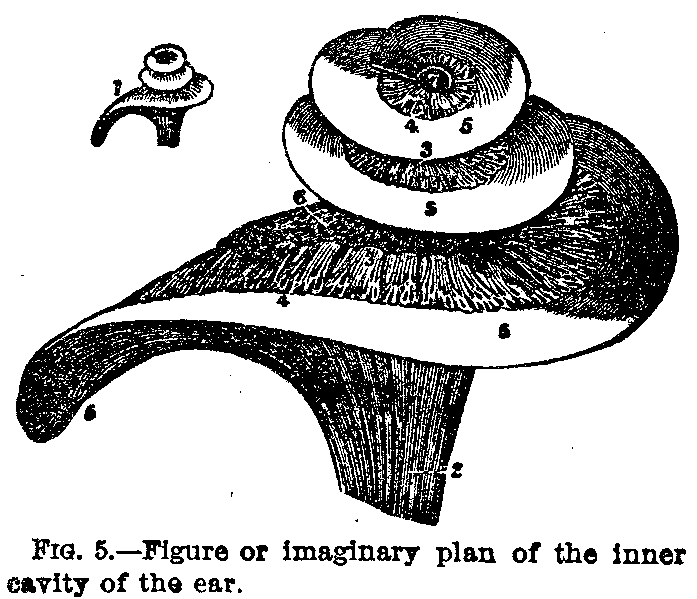
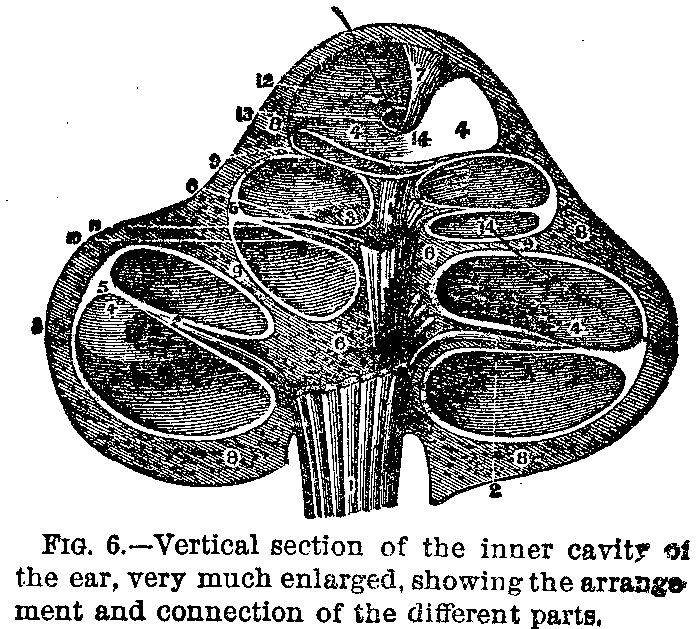
FIGURE NO. 1.
1, 2, 3. The inner cavity open, showing the spiral lamina.
4, 5, 6. Rest of the cells of the inner cavity.
7, 8. Vestibule.
9, 10. Upper canal.
11, 12. Lower canal.
13. Outer canal.
14, 14. Semicircular membranous canal.
15,16,17. Acoustic or auditive nerve.
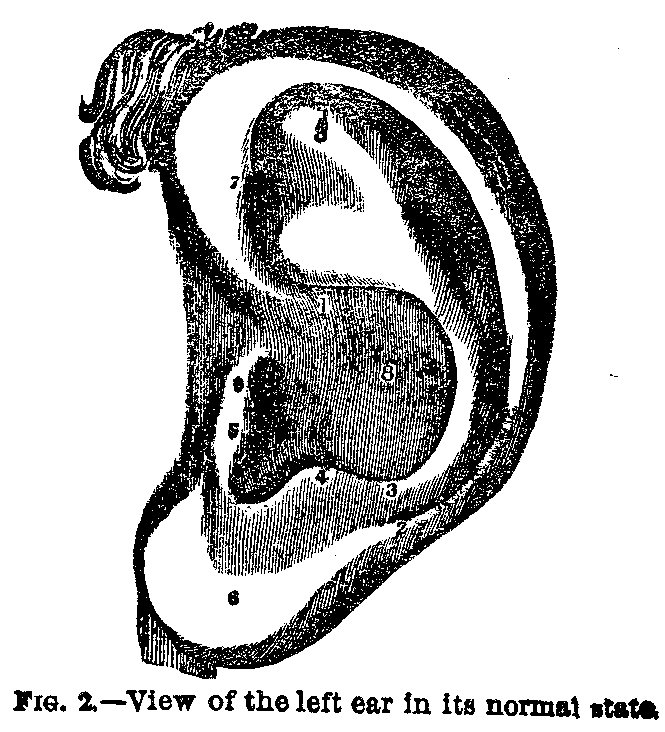
FIGURE NO. 2.
1, 2. Origin and end of the helix.
3. Antihelix.
4. Antitragus.
5. Tragus.
6. Lobe of the outer part of the ear.
7. It points to the navicular pit, and is in front and
over the wing.
8. Shell.
9. Outer auditive due.
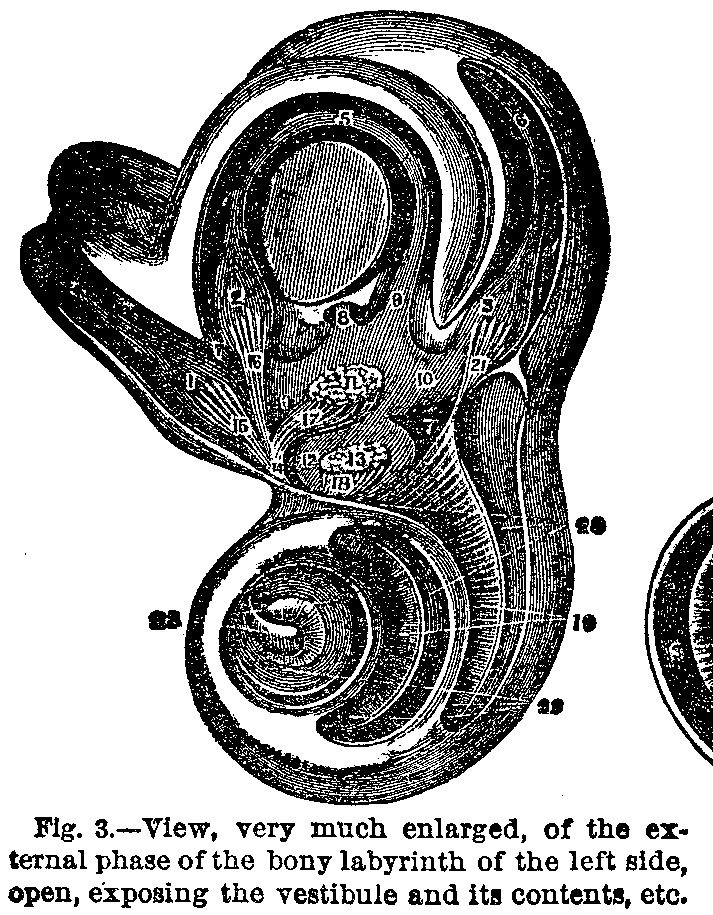
FIGURE NO. 3.
1. Swelling of the upper semicircular canal.
2. Swelling of the outer canal.
3. Swelling of the lower canal.
4. Upper semicircular membranous canal.
5. Outer membranous canal.
6. Lower membranous canal.
7. Spaces between the semicircular membranous and bony canals,
supposed to be filled with coatunni humor.
8. Common due formed by the union of upper and lower membranous
canals.
9. Place where the inner semicircular canal opens into the
elliptical urn of the vestibule.
10. Elliptical urn which contains the:
11. Breschid otocones.
12. Spheric urn containing also some:
13. Otocones.
14,15,16,17,18. Expansions of the acoustic nerve to the membranous
canal and the elliptical urn, and also the spheric.
19. Turns of the spiral lamina.
20. Ladder of tympanum.
21. Nervous expansion to the back swelling.
22. Vestibule ladder.
23. Modiolum.
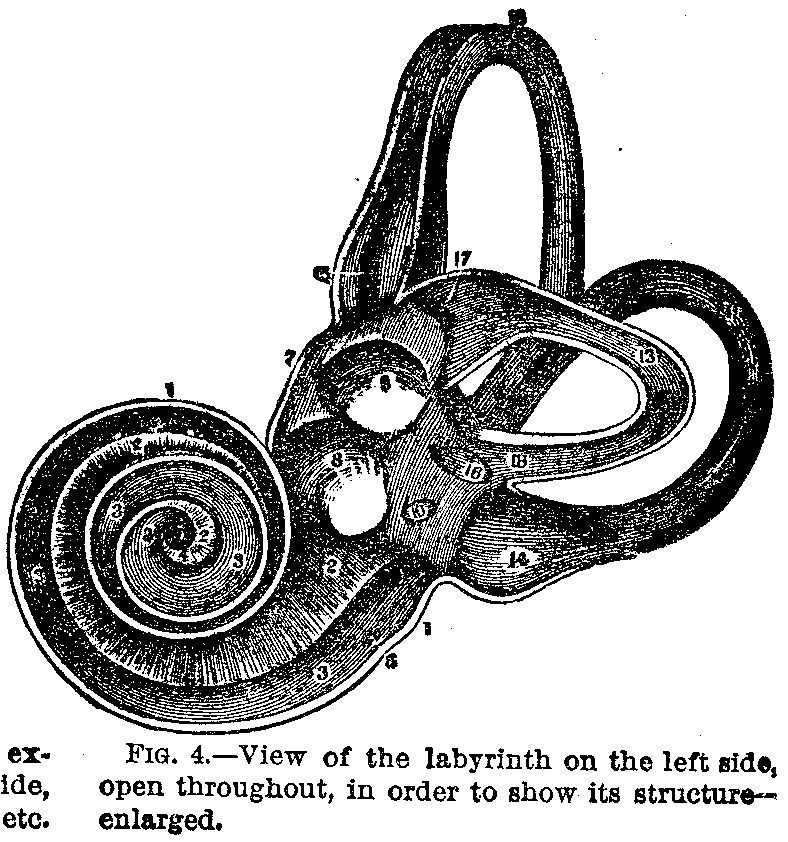
FIGURE NO. 4.
1. Thickness of outer covering of inner cavity.
2, 2. Vestibule ladder or upper cover of the spiral lamina.
3, 3. Tympanum ladder or lower cover.
4. Hook of the inner cavity.
5. Centre of the infundible.
6. Round opening communicating with the tympanum.
7. Thickness of the outer cover of the vestibule.
9. Oval opening.
10. Orifice of the aqueduct of the vestibule.
11. Lower semicircular canal.
12. Upper semicircular canal.
13. Outer semicircular canal.
14. Swelling of the lower canal.
15. Swelling of the upper canal.
16. Common orifices of upper and lower canals.
17. Swelling of the outer canal.
FIGURE NO. 5.
1. Normal size. The other is much enlarged.
2. Zone of acoustic nerve.
3. Arrangement of filaments In the vesicular zone.
5. Membranous zone.
6. Bony texture of the modiolus.
7. Opening between the two ladders.
FIGURE NO. 6.
1, 1. Zone of the acoustic nerve.
2, 2. Filaments of the same in the bony zone.
3, 3. Anastomosis in the vesicular zone.
4, 4. Membranous zone.
5, 5. Fold of outer edge.
6, 6. Axis of inner cavity.
7. The mediolus.
8, 8. Outer bony walls of the inner cavity.
9, 9. Bony layers of the spiral lamina.
10. Vestibule ladder.
12. Hook of the inner cavity.
13. Infundible.
14. Horse hair passed through the course of the spiral lamina.
|
|
|
|
|
|
|
For an explanation of the illustrations see text on opposite page.
|
|
|
|
|
|
|
Number of Diseases.—The number of diseases of the ear is twenty-four, but as a majority of them require for their recognition and effective treatment more or less peculiar and costly apparatus, only a few of the most important require notice in this chapter. For the understanding of these, however, a brief review of the anatomy of the ear is necessary.
Anatomy of the Ear.—The external ear, or auricle, as anatomists call it, is supposed by many people to be the chief part of the organ of hearing, but in reality the essential pieces lie inside the head, some, indeed, imbedded in the most solid bone of the skull, and one so hard that it is has received the name of the petrous or rocky portion of the temporal bone.
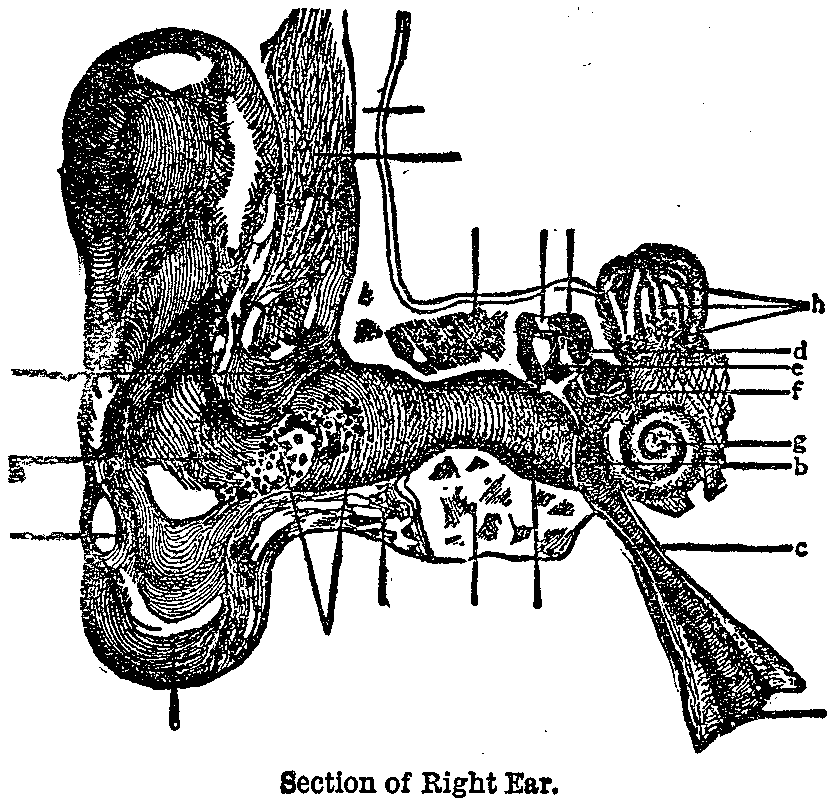
Auditory Canal.—Besides the auricle, which is all that portion of the ear projecting from the head, the external ear is considered by anatomists to include the auditory canal (a) or opening into the head, and the delicate tympanic membrane or drumhead (b), which is drawn across the auditory canal like a curtain, at a depth of about one inch and a quarter from the outside.
The Ear Drum.—The middle ear, as it has been named, called also the drum of the ear, is bounded outwardly by the tympanic membrane, and inwardly by the bony portion of the labyrinth or internal ear. It includes the Eustachian tube (c), which is a fleshy pipe, communicating through the head with the upper and back part of the throat, and it contains the ossicles or little bones of the ear (d, e, and f).
Ossicles or Little Bones.—These ossicles are three in number, and are named from their resemblance to the familiar objects after which they are called—the hammer (d), the anvil (e), and the stirrup (f). These remarkable little bones play a curiously elaborate part in this mechanism of hearing.
|
|
|
|
|
|
|
The Labyrinth.—The chief portions of the internal ear, or labyrinth, as it is often called, on account of its perplexing structure and function, are the cochlea or snail-shell (g), and the semicircular canals (h). The appearances of these are sufficiently indicated by their names, and their positions can be best understood by looking at the adjoining picture.
Use of the Auricle.—The object of the auricle in man is to collect the waves of sound, just as the broad mouth of an ear-trumpet does, and it seems to have no other duty in the process of hearing. In order to prevent, as far as possible, the entrance of insects with the sound-waves into the auditory canal, the exterior opening of this tube is guarded by stiff, coarse hairs.
Ear-Wax.—It is also generally covered with a sticky, bitter substance, the ear-wax, secreted by numerous ceruminous glands (i), apparently to stop, or disgust, any adventurous creatures which may attempt to make their way in toward the drum. This provision is highly necessary, because the tympanic membrane is so exceedingly sensitive that a very slight touch, even from the foot of a small insect, would cause intense pain.
Delicacy of the Drum.—On account of this great delicacy of the membrane of the drum, it is unsafe to put any hard object into the ear for the purpose of cleansing it. Hence, the corner of a towel is far better to wipe out the ear with than an earpick or any other solid instrument..
Wax Plugs.—Sometimes a firm plug of wax accumulates in the external auditory canal, and causes deafness, which, however, can be entirely and immediately cured if the hardened wax is removed by syringing with warm water.
Foreign Objects in the Ear.—When children put beads, grains of corn, and so forth, into their ears, no attempt should be made to pick them out with hair-pins or bodkins, lest, on the contrary, they be pushed further down the tube. It is much wiser to send for a physician, who is provided with suitable, delicate forceps, for removing them without risk of such a serious addition to the original misfortune.
Insects in the Ear.—If an insect makes its way into a person's ear, notwithstanding nature's safeguards against such an accident, the patient should at once lie down on the opposite side and have the affected ear filled up with sweet olive oil, which will probably kill the creature and cause it to float up to the mouth of the auditory canal, where it can be picked out.
|
|
|
|
|
|
|
Office of Auditory Canal.—The office of the auditory canal is to convey sounds, after they have been collected by the auricle, to the drum-head, which is caused to vibrate just as that of a soldier's drum does when it is beaten, or rather as the sounding-board of a piano does when the keys are struck. The vibrations thus produced are transmitted along the chain of ossicles, that is to say, the handle of the malleus or hammer, being fastened to the tympanic membrane, moves with it. In thus moving, it tilts the incus or anvil slightly over, and this motion of the anvil in its turn causes a slight oscillation of the stapes or stirrup.
The Stirrup.—But the stirrup is fastened by its foot-plate to the membrane covering a little hole in the bony wall of the labyrinth, called the oval window, so that any vibration of the drum-head or tympanic membrane is carried along over this chain, or bridge of bones, to the covering of the oval window. Behind this latter membrane the whole labyrinth is filled with a watery fluid, which bathes the terminations of the auditory nerve in the cochlea.
The Semicircular Canals.—The exact use of the semicircular canals is not understood, but there is little doubt that the fine hairs proceeding from cells found in the cochlea are thrown into vibrations by undulations transmitted from the membrane of the oval window through the fluid contained in the cavities of the labyrinth. Then these vibrations of sound are perceived by the delicate nerve-fibres, in which the auditory nerve terminates, very much as the undulations which constitute light and color are perceived by the filaments of the optic nerve, where they terminate in the rods and cones of the retina. Obviously, with such a complicated and excessively delicate mechanism for carrying on the process of hearing, the wonder is, not that few people hear imperfectly, but that everybody is not as deaf to all sound as the world has been in previous ages to the teachings of hygiene.
Ear Tumors.—This outer part of the ear is the occasional seat of gouty and other deposits, which give rise to prominences and irregularities of its surface; it may also be affected with a kind of vascular tumor called haematoma, and still more frequently be the seat of benignant and malignant or cancerous tumors, and of various malformations.
Sizes of the Ear.—In persons of slight and delicate organizations, with a scanty stock of vitality, the outer ear is often exceedingly small, although it may be perfectly shaped. In persons of large build and actively circulating blood, the auricle is sometimes relatively large, the lower lobe being pendulous and of exaggerated development.
|
|
|
|
|
|
|
What Large Lobes Indicate.—As a rule, a large lobe of the ear indicates a free vascular supply of blood to the brain, and is said to be to some extent a sign of epilepsy, and of other kindred nervous diseases.
Danger from Earrings.—If people choose to run the risk of suffering from the dangerous little tumors which are sometimes caused by the barbarism of wearing earrings, they should be very careful to diminish the chance of injury as much as possible by having the auricle pierced with a clean, bright instrument, and by preventing the cartilage, which sometimes comes quite low down in the lobe of the ear, from being wounded.
Boxing and Pulling Ears.—Children should never be punished by "boxing" or pulling the ears. The former piece of brutality might instantly burst the tympanic membrane, causing deafness for life, and the latter is liable to originate severe inflammation of the auricle, leading to the same unfortunate result.
Symptoms.—The symptoms of this affection are the same as of acute eczema and the reader is referred to the article on that subject. There is also a chronic form in which the skin is thickened and crusts are formed.
Causes.—1. Detention, when it is due to nerve-irritation.
2. Discharges from the ear which irritate the auricle.
3. Hoods by pressing the auricle against the side of the head and preventing the evaporation of the perspiration.
4. A chronic form sometimes found in old people is due, likely, to a weakened "tone" of the tissues.
Treatment.—The treatment is the same as in eczema of other parts of the body. Where it is possible, the cause should be removed. Cleanliness is essential but water is contra-indicated and the crusts should be removed by olive oil. The ammoniated mercury ointment, which is official and to be had at all drug stores, should be applied twice daily after thorough cleansing. Cod-liver oil and iron are often of use as internal remedies.
Definition.—This is a swelling of the auricle in which there is an infusion of blood between the cartilage of the auricle and the perichondrium. It is frequently caused by traumatism and often occurs in the insane.
|
|
|
|
|
|
|
Symptoms.—The symptoms are swelling and slight pain.
Treatment.—Gruber recommends, if the blood is coagulated, incising the tumor and removing the clot. Painting -with tincture of iodine ia advised for the thickening. Cold or warm applications may be tried to relieve the pain.
Character.—This is one of the most painful maladies that flesh is heir to. It is rendered so frightfully painful by the fact that it is shut in between a layer of strong cartilage and solid bone. Probably the most common cause of abscess in the ear is taking cold, although picking the ears with hard, sharp instruments sometimes seems to excite it. As it is impossible to tell which side of the auditory canal the abscess is going to form, early in the case, lancing must be deferred.
Treatment.—As a rule, all that can be afforded in the way of relief, is gained by hot poultices made out of ground flaxseed, bread and milk, or little bags of hops dipped in hot vinegar and changed very frequently, or as soon as they grow cool. As soon as the abscess is well localized it should be opened by a physician, thereby relieving the patient of a great deal of suffering. In the meantime some respite and sleep may be obtained by the use of opium suppositories containing one grain each used every four hours, or hypodermic injections of one-eighth to one-half of a grain of morphia.
Causes.—An exostosis or bony tumor occasionally springs from the walls of the auditory canal, pushing the mucous lining before it, and filling up part or all the calibre of the tube. It is most frequently met with in people of a rheumatic or gouty tendency. Until chiseled away, it is sometimes very painful, and a serious obstacle to hearing.
Causes.—This is the name given to that condition in which the canal is partially or completely filled with ear-wax. The wax may be very hard and may be mixed with dirt and dust. It is caused sometimes by the shape of the canal, and on the other hand is often due to one's occupation.
|
|
|
|
|
|
|
Symptoms.—Deafness, dizziness and buzzing in the ear are frequently complained of, but to make sure that impacted wax is present it should be seen. It appears as a dark mass in the canal.
Treatment.—If the wax is soft, it may be removed by repeated syringings with warm water. If it is hard, the canal should be filled with warm olive oil and then the syringing tried. An instrument of any kind should never be introduced into the canal for its removal by the unskilled hand.
Symptoms.—Inanimate foreign bodies, such as beads, buttons, grains of corn, etc., give rise to the same symptoms as impacted wax. In the case of grains, water tends to swell them and so makes their removal more difficult. In such cases the surgeon should be called upon.
Use of Syringe.—Insects occasion great pain which may simulate intense neuralgia, or, by a reflex action, may refer the pain to the teeth and so lead one astray. The syringe should be used and hot water is very grateful to the patient, soothing the inflamed part.
Character.—Inflammation of the drum-head is an acutely painful affection, sometimes attended with fainting fits in its early stages, and usually resulting in deafness because the membrane is left thickened, and therefore incapable of properly responding to the vibrations of sound.
Treatment.—Leeching, followed by blisters behind the ear, or on the nape of the neck and opium internally or hypodermically, to mitigate the suffering, which is often very severe, will prove of great value. Hot applications to the ear in the shape of bags of hops, a stove lid wrapped in flannel, or the hot-water bottle may be sufficient to give relief.
Treatment of Children.—In young children a hot foot bath will relieve by dilating the small blood-vessels of the lower extremities and so drawing some blood from the inflamed area. As hot water as can be borne may be dropped into the ear. With the best of care we will frequently be rewarded by
Causes.—This is especially liable to occur during the course of scarlet fever from suppuration of the middle ear, and if neglected leads to permanent deafness. Hence, in scarlatina, the ears of a child should be carefully examined daily with the little conical ear-speculum, if there is the slightest complaint of pain in them, in order to prevent this disaster by early puncture of the drum-head, which allows the escape of the imprisoned pus, and so saves the organ of hearing. Still, when the perforation remains in the drum-head the auditory sense is often only slightly unpaired.
|
|
|
|
|
|
|
Treatment.—Suppurating or running ears need, above all things, that cleanliness should be maintained as much as possible. If pus remains in the middle ear, a chronic inflammation is kept up and normal tissue is destroyed—eaten away as one might say. Hearing becomes more and more difficult and life is constantly in jeopardy, for the bone may become affected and the brain finally exposed to infection and a brain-abscess develop. Cleanliness may be maintained usually by washing out the ear with a hot solution of carbolic acid two or three times daily. A two per cent. strength is sufficient. If this fails to cure the ear, which would be evidenced by a cessation of all symptoms, especially pain and discharge, a specialist should be at once consulted. Dead or necrosed bone may be present, or granulation tissue—"proud flesh,"— and should be removed as soon as possible.
Thickening of Tympanum.—Thickening and condensation of the tympanic membrane are liable to occur in advanced life, the delicate skin forming the drum-head undergoing a slow process of change, by which it loses its elasticity and becomes firm and hard almost like the nail of the finger. Of course, in this condition the vibrations into which it should naturally be thrown are rendered very imperfect, and the hearing is correspondingly defective in old people who are the subjects of this degeneration.
Causes.—The Eustachian tube is liable to inflammation from extension of disease from the throat, even such a simple irritation as that of a common cold. It is also subject to obstruction and contraction, so that the air cannot pass freely through it into the cavity of the tympanum, as it should do in health. When this takes place, the vibration of the drum is interfered with, there is pressure within the cavity, and consequently a sense of fullness and deafness is experienced, which is very oppressive.
Treatment.—This distressing condition can often be greatly relieved by calling in a skillful aurist, who may pass a probe or hollow tube along the Eustachian canal into the middle ear, and so restore the communication of the latter with the external air.
|
|
|
|
|
|
|
Diseases of the Middle Ear.—Diseases of the middle ear and of the internal ear comprise inflammation, ulceration and abscess. All these are very painful, difficult to recognize with certainty, and, as a rule, beyond the power of any but the most skillful treatment. In every case an experienced aurist should therefore be immediately called in, and until he arrives the severity of the pain may, perhaps, be held in check by some of the means suggested when speaking of abscess of the auditory canal.
Anatomy of the Hose.—The organ of the sense of smell is much more extensive than people who have never studied anatomy imagine. Instead of being merely a triangular projection of some two or three inches long, and an inch or an inch and a half high, occupying the middle of the face, it is a large double cavity reaching far back into the head, and communicating by the posterior nares or hinder nostrils with the upper part of the throat. The external portion of the nose is composed at its upper third of small bones, which are continued at its lower part by plates of cartilage.
Nose Bones and Cartilages.—These cartilages and bones are covered on the outside with a thin skin, and on the inside with a mucous membrane, which in the deeper recesses of the cavity is identical and continuous with that of the mouth and throat. The external division between the two nostrils is carried upward and backward by a flat, very thin bone named the vomer; and the sides of the two cavities, which are continuous with the exterior nostrils, are partly filled up with soft, spongy processes of bone, three of which are called the turbinated bones, because they are rolled up like a scroll.
The Mucous Membrane.—These turbinated bones are covered, like the rest of the nasal cavities, with a mucous membrane, named the Schneiderian membrane, richly supplied with blood-vessels, which approach very near its soft and delicate surface. It is from these small, but active, little blood-vessels that the hemorrhage usually comes in bleeding from the nose.
The Olfactory Nerves.—The nerves of smelling, called the olfactory nerves, enter the upper part of the nose through openings in the sieve-like bone, which forms the roof of the nasal fossa. After passing into the nose, these olfactory nerves divide up into a great number of tiny branches, which run along under the surface of the Schneiderian membrane, and are spread out upon the superior and middle turbinate bones, and on the sides of the partition between the two nasal cavities. The great use of the turbinated bones and processes is to furnish a large extent of surface upon which these branches of the olfactory nerve can be expanded.
|
|
|
|
|
|
|
Functions of the Olfactories.—And this spreading out of the olfactory nerve is evidently in order that the sensitive filaments may, on occasion, come in contact with as large a number as possible of the exceedingly minute, odorous particles which many substances, such as musk or camphor, are constantly giving off in such abundance.
How We Smell.—These odorous particles have the power of affecting the terminal filaments of the olfactory nerves in different ways, which we recognize as the agreeable or disagreeable odors of the objects from which they originate. The excessive minuteness of such particles may be comprehended from the fact that the apartment of the Empress Josephine in one of the French Imperial palaces was found, after twenty-four years of disuse, to give off a distinct odor of the musk employed by that unfortunate lady when she occupied it.
Uses of the Sense of Smell.—The power of distinguishing odors, which to some animals, including all those beasts which pursue their prey by scent, is one of the most vitally important, chiefly serves as a means of gratification or its opposite to human beings.
Hygienic Office of Smell.—But although the sense of smell does not in civilized communities contribute anything toward sustaining life by helping us to secure food, it has a very useful hygienic office, which should never be forgotten, in guarding us against some of the most common and dangerous causes of disease, in foul air and polluted water.
Nose as a Warming Organ.—Besides this the nose has an important work to do in warming and, to some extent, purifying the air we breathe, as that air is drawn through the narrow and winding passages among the turbinated bones. The Schneiderian membrane over which this air passes being generally moist, and more or less covered with adhesive mucus, helps to catch not only the odorous particles, but larger and more hurtful impurities, and so is quite mechanically a valuable protector to human health.
Causes.—Nose bleed may be due to a blow, picking the nose, the presence of a foreign body in the nose, or to the use of instruments in the nose. Diseased conditions within the nose often occasion it. In girls it may replace the natural menstruation. Diseases of the heart, liver and kidneys may give rise to it.
|
|
|
|
|
|
|
Treatment.—In cases of slight bleeding, pressure or the snuffing of ice-water may suffice. If these fail, cotton dipped in a one to ten thousand solution of adrenalin, should be packed into the nostril and kept there for ten or fifteen minutes. Iron, tannic acid and alum—the remedies our grandmothers used, are now supplanted by this modern drug which does not irritate the delicate lining of the nose as the old remedies did. If the adrenalin solution does not check the hemorrhage, it may be necessary for the physician to plug up both the anterior and posterior nostrils by the aid of an ingenious little instrument which has been devised for that purpose.
Forms and Causes.—"Catarrh" is a word derived from the Greek word katarheo, meaning to flow down, and is used in medicine to designate a particular form of inflammation of the mucous membrane. It has many forms and is due to many causes, and no one has ever found nor ever will find one remedy for "catarrh." This truth should be better and more generally known by the intelligent public.
Causes.—As causes of "catarrh" may be mentioned:
1. Climatic influences. Many patients lose their catarrh when they change from one climate to another.
2. Inherited predisposition. One cannot inherit catarrh, but the weakness of the mucous tissues may be inherited and so predispose to the affection.
3. Indigestion, constipation, intestinal parasites (worms), heart, lung, liver and kidney diseases are often provocative of a catarrhal state of the nasal mucous membrane.
4. Many fevers at their beginning or during their course are accompanied by acute catarrhal disturbance. Typhoid fever, measles and scarlatina are examples.
5. Deformity within the nasal chambers is one of the most frequent factors, and local remedies are of no avail as far as a permanent cure is concerned. In these cases the only sensible treatment is the correction of the deformities, thus bringing the organ into a condition as near the normal as possible.
Catarrh as the Cause of Tuberculosis.—There is a general belief that catarrh is to blame for the great majority of the cases of consumption. This needs some modification before it is to be accepted. Surroundings, family predisposition, climate, and weak, non-resisting tissues are as much to be blamed for the occurrence of this terrible malady. Catarrh does, however, play some part as a factor.
|
|
|
|
|
|
|
Liability of Infection.—Professor Osler, of Johns Hopkins University, says on this subject: "The liability of infection in the cervical and bronchial glands in children is probably associated with the common occurrence of catarrhal processes in the throat and bronchi." This means that neglect of catarrhal conditions in a child makes that child more likely to be infected with tuberculosis, and if the family has a history of tuberculosis there is all the more reason for thoroughness of treatment of the existing catarrhal condition.
Dr. Lartigau's View.—Dr. Lartigau, of New York, in his article on tuberculosis in the Twentieth Century of Practice of Medicine, under predisposing conditions mentions susceptibility to catarrhal inflammations.
Character.—This is a term applied to a form of catarrh characterized by a horrible and peculiar stench and the formation in the nose of crusts of dried secretions upon which the fetor depends.
Causes.—In some cases it is due to a constitutional disease, as syphilis. In the majority of instances, however, it is the continuation of a catarrhal inflammation, in which the mucous membrane shrinks—atrophies—and the secretions therefrom are changed, becoming more tenacious and concentrated.
Symptoms.—These are the crusts and the peculiar fetor mentioned above.
Treatment.—Cleanliness is the great sine qua non—a fact easily remembered when one realizes that the fetor is from the decomposing crust. To detach the crusts various washes have been prescribed. A solution of bicarbonate of soda is a good solvent and may be prescribed as follows:
Rx.---Bicarbonate of soda.......................... 2 ounces
Common table salt............................ 1 ounce
Menthol ..................................... 4 grains
Mix. Directions: Half a teaspoonful in a cup of warm
water, snuffed up the nose until the nostrils are clear. Use
twice daily.
Or
Rx.---Bicarbonate of soda.......................... 2 ounces
Biborate of soda............................. 1/2 ounce
Salicylic acid............................... 1 drachm
Menthol ..................................... 4 grains
Mix. Directions: Same as for preceding prescription.
|
|
|
|
|
|
|
Or
Rx.---Dobell's Solution.
Dilute with three or four parts of warm water and use as
a nose wash.
Steam Inhalations.—If these washes are not effectual in removing the crusts steam or hot vapor inhalations may be tried. In obstinate cases it is often necessary to remove the crusts with some force, either with cotton on a probe or with forceps. After the crusts are gotten rid of, antiseptics and deodorizants should be employed. Weak solutions of potassium permanganate, bichloride of mercury, and when the patient can stand the pain, a one-half to a one per cent. solution of formaldehyde.
Removal of Dead Bone.—When the fetor is due to dead bone, the dead bone should be at once removed.
Treatment of Syphilitic Catarrh.—If a syphilitic taint, either inherited or acquired, is the foundation of the odor, proper constitutional treatment should be instituted at once and maintained until long after the nasal symptoms have disappeared.
Causes.—Nasal polyps are grape-like tumors which are dependent from the upper and outer wall of the nose—on the inside—and are supposed to be one of the possible results of chronic inflammation of the lining mucous membrane. They are rarely seen before the fifteenth year.
Symptoms.—When small they may present no symptoms. If they are large, they may cause obstruction to the respiration, pervert the nasal secretions, cause headaches, give a nasal twang to the voice, and, in some cases, undoubtedly provoke asthmatic attacks.
Treatment.—The treatment is removal, which may be accomplished by twisting the tumor free from its attachment, by cutting it at its base, or preferably by using a wire snare.
Nature.—This is a skin disease affecting usually the skin-covering of the nose, is chronic, and is characterized by redness, thickening of the skin, and more or less acne.
Causes.—These are various. According to Prof. Van Harlingen, "in early life it is generally due to anemia and debility, nervous prostration or dyspepsia. In later life the use of spirituous liquors is often the cause, and, perhaps nearly as often, dyspepsia in some of its forms." In women, disturbances of the menstrual function, even pregnancy, may act as a causative factor.
|
|
|
|
|
|
|
Treatment.—To be successful persistence in treatment is often necessary. The first thing to be done is to remove the cause. "Uterine and menstrual derangements are to be looked after, the stomach and bowels kept in good order, and all hygienic measures used to improve the general health. Alcoholic and malt liquors are to be totally eschewed. Tea and coffee should be drunk in moderation and not strong. Inveterate tea drinkers are very apt to have red noses."
The Favorite Drug.—The favorite drug both for internal and external use in this disease is ichthyol. Internally it may be administered in peppermint water, equal parts of each, ten drops being the dose and given every four to six hours. Locally it may be used as an ointment or as a paint:
Rx.---Ichthyol ...................................... 1 drachm
Subnitrate of bismuth.......................... 1 "
Ammonlated mercury............................. 1 "
Vaselin ...................................... 10 drachma
Mix. Apply freely before retiring. (Dr. Latoir.)
Rx.---Ichthyol ...................................... 1 ounce
Oil of eucalyptus........................... 10 drops
Oil of bergamot.............................. 5 "
Mix. Paint on at night; wash off in morning with soap and
warm water; then apply dusting powder. (Merk.)
Vleminck's solution is recommended by Stelwagon, diluted one to ten parts of water. The formula for the strong solution is:
Rx.---Calcis ....................................... 1/2 ounce
Sublimed sulphur............................ 1 "
Water ....................................... 10 ounces
Boil down to six ounces and filter. Apply locally three or
four times a day.
Treatment of Obstinate Cases.—In obstinate cases regular treatment at the hands of a skilled specialist is necessary, and the earlier the case applies to him the more likelihood there is of his affecting a cure. The treatments outlined above are those most in favor with noted specialists and most likely to reward the efforts of the amateur physician.
Treatment.—Warts in this locality are often mistaken by the laity for cancer and afford the charlatan and the advertising doctor an opportunity to make "cures" of this greatly feared disease. Warts in this locality are treated just as in other parts of the body.
This page is maintained by
Charles Keith.
Contact:
Send me a message
Last Modified: Monday, 13-May-2013 15:31:46 EDT